|
If you're going to get a lot of IV drugs
sometimes they'll suggest a port, and this is a glorious, glorious
thing. The reason that an implanted port is so fabulous is
that it sits just under your skin and connects to a much larger vein
than the ones generally accessible to a normal IV so instead of
butchering my arm on a weekly basis by repeatedly looking for a
decent vein and then proceeding to devastate it the nurses can
simply plunge a needle into the port and start the IV right away.
I wish I had realized how wonderful the implanted port would be
before the chemotherapy damaged the veins in my arm, but hindsight
is 20/20, so I hear.
I specifically requested to stay awake for
this surgery; normally it's done under a general anesthetic. I
now know why most people are put under for this procedure... even
though the local anesthetic was very effective there was still quite
a bit of bone and muscle manipulation and there were a couple of
times when the pain was fairly intense (you can get some idea of the
manipulation involved by looking at the residual bruising in the
final photographs). I'm still glad I stayed awake for this
one, though, since I would always rather know everything that
happens. It's also nice to just be able to drive home from the
hospital, although it took some explaining to convince the recovery
nurses that I'd only been under a local anesthetic, heh.
|

I'd hoped that this would be
the last IV I would have in my arm for a long, long
time, which is why I bothered to take a photograph
of it. Much to my dismay, however, I have
since learned that most emergency rooms and similar
environments do not like to access a port and there
are a lot of medical procedures that require a
different sort of IV speed or volume than a port can
supply. Balls.

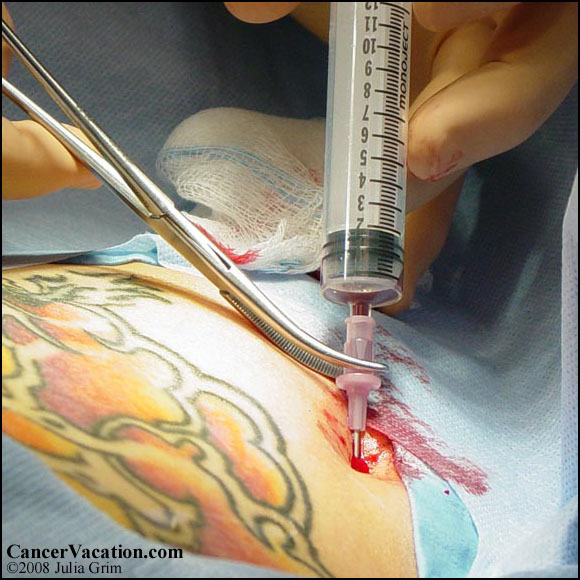

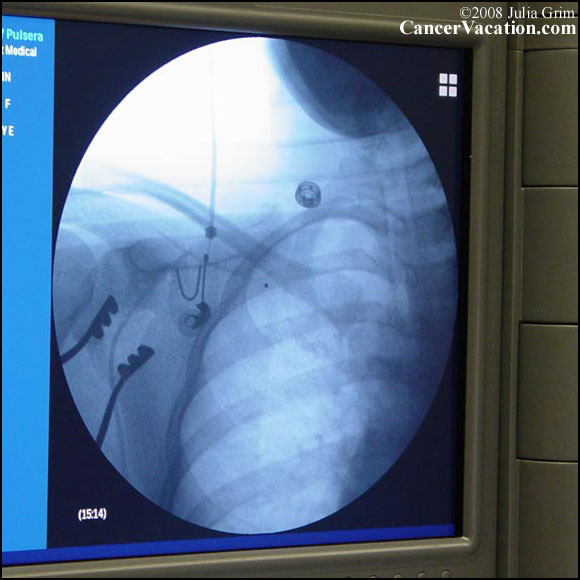
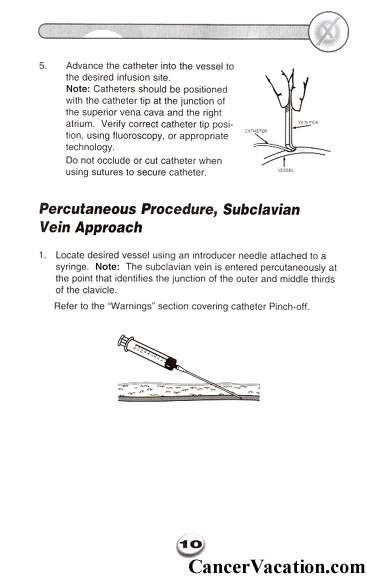
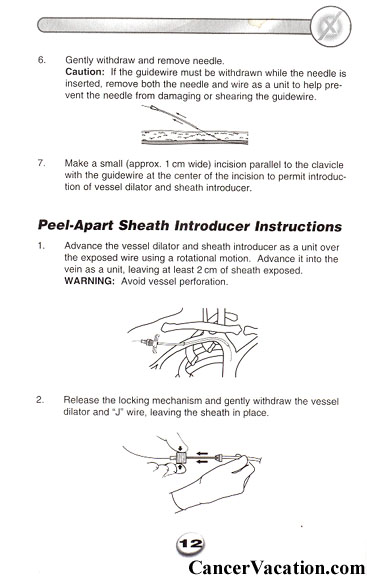
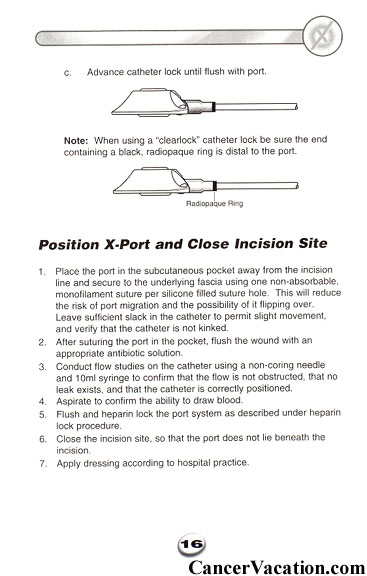
At the bottom of this page
I've included some information from the "instruction
manual" that hospitals receive with this kind of
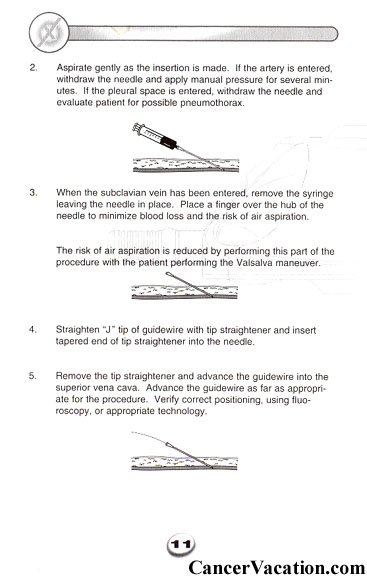
port... you can read there that the vein is accessed
by first running a guide wire through the vein and
then replacing it with the appropriate tubing.
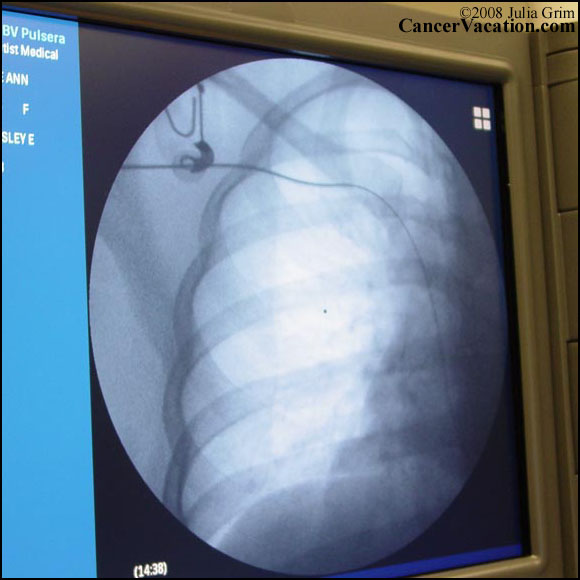
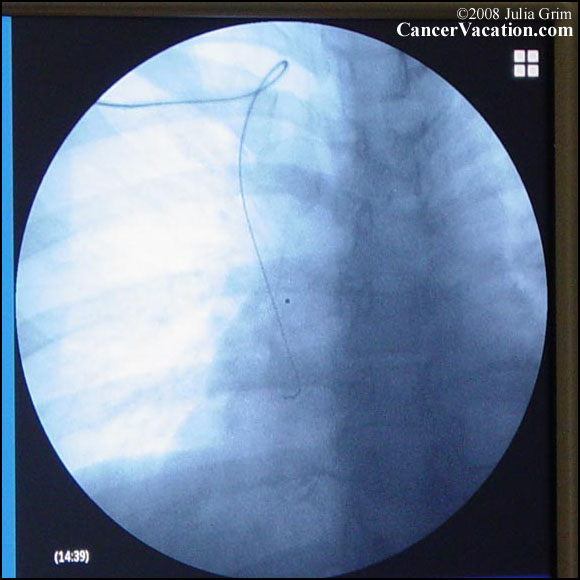
The whole time they were
working on me on the table they were also able to
see exactly where the guide wire was located by
looking at a giant X-ray screen on a nearby wall.
The amount of precision needed to manage this is a
little intimidating.
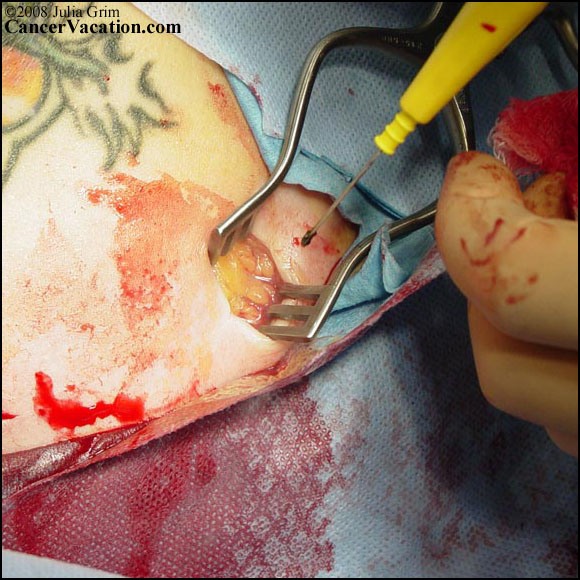
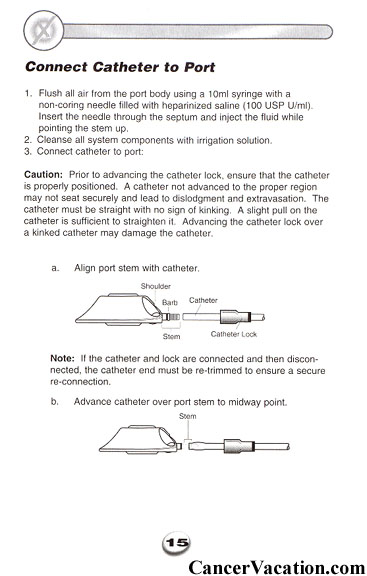
I always wondered where those
salad tongs went...

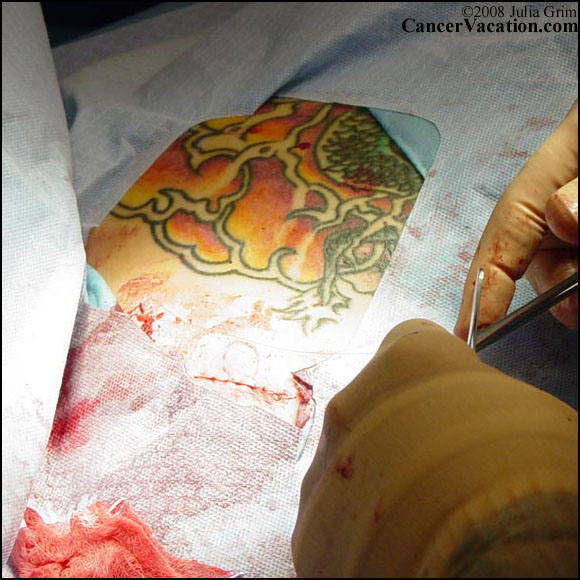
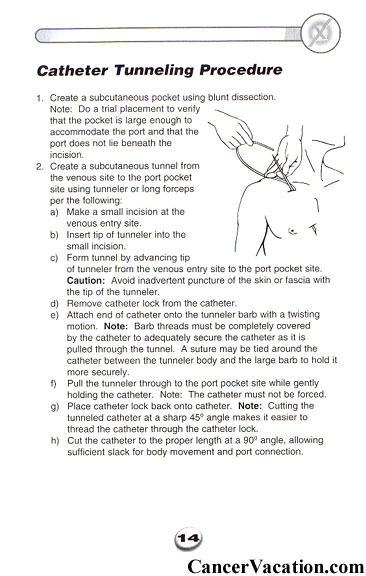
This is what the implanted
port looks like and approximately where it sits,
although you can't see it once they close the
incision. The skin covering the port is very
thin, though, and you can pretty much feel the whole
thing with your fingertips and even see it if you
turn your head or shoulders the right direction.

I really was awake for the
whole procedure... I just had my eyes screwed shut
in this photo because of some momentary pain.

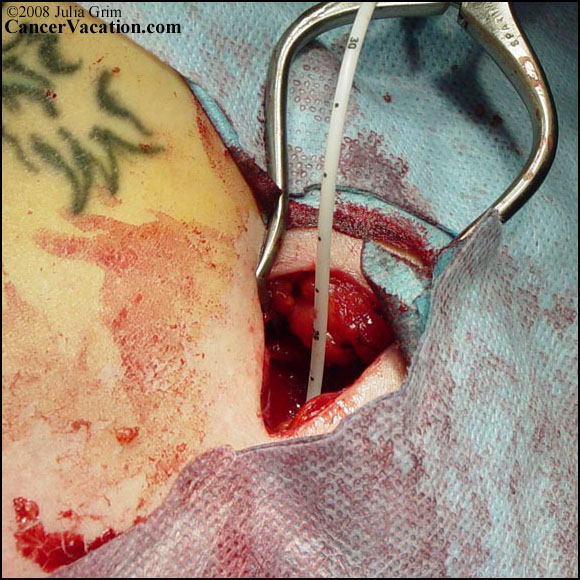
There is a suspicious lack of
salad tongs on this table...

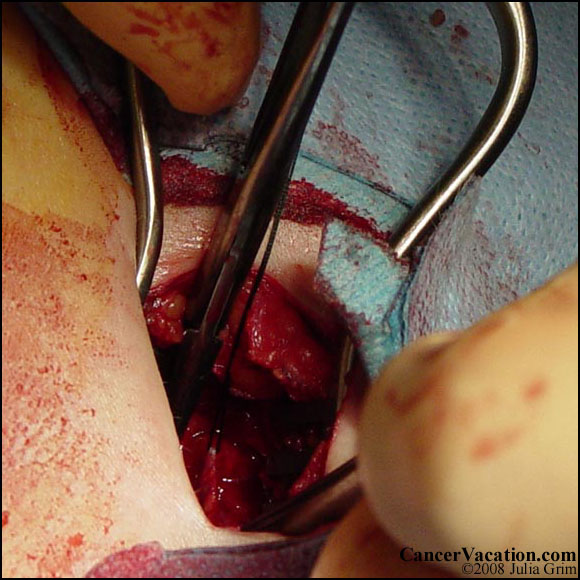
Both this photograph and the
one following do a tremendous job (in my opinion) of
demonstrating how much muscle and bone manipulation
were involved in placing the port. There were
times when the pain in my shoulder and collar bone
was very intense indeed, and you can see that the
end result here is a lot more traumatized (in
appearance at any rate) than even the mastectomy
was.

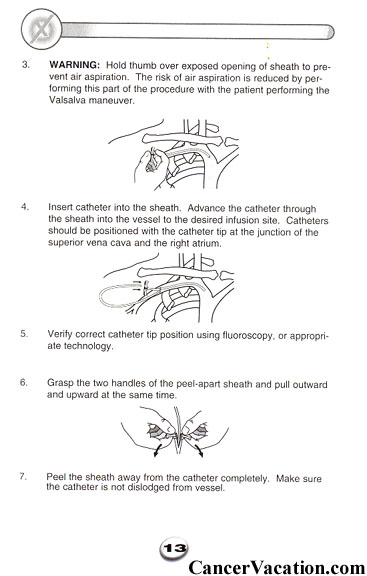
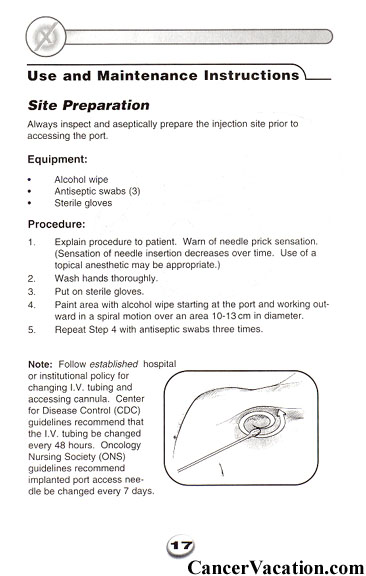
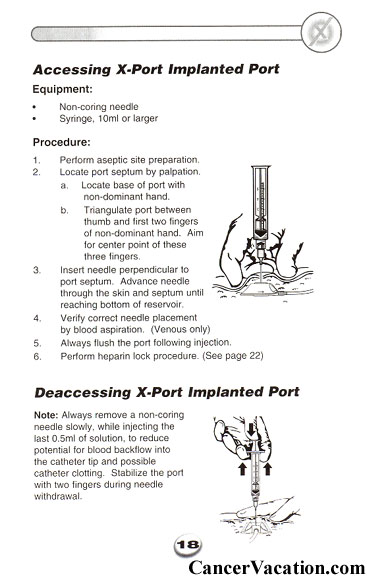
The following images are from
the instruction manual that came with my implanted
port... this isn't a piece of literature that
patients normally receive but the nurses thought I
might want it to go with my surgical photos and they
were right. It helps to explain some of the
installation (is that the right word?) process and
gives a fairly good view of what the actual port
looks like and how it functions:
|
|